|
Introduction
Case1:
Vomiting
Case 2:
Cough & fever
Case 3: Bruising
Case 4: Sore
throat
Case 5: Jaundice
Case 6: Flu & fever
Case 7: Diarrhea
Case 8: Black
Robe
Case 9: Back Pain Catching the
beast
Thanks to
Quiz
Please |
|
More fascinating
stuff about malaria.
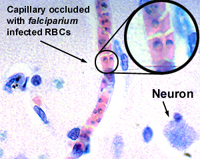
- RBCs infected with P. falciparium
develop little 'knobs' on the membrane surface.
- These knobs bind to ICAM-1 receptors on
the capillary and venule endothelial cells.
- This is the disaster of cerebral malaria.
- Not growth of the bug in the
brain.
- Rather, small vessel occlusion.
- The picture to the right shows this.
- Intermittent bouts of RBC hemolysis lead
to:
|
 |
- The characteristic spiking and remitting
fever pattern.
- Massive loss of hemoglobin in the
urine, so-called 'black water fever.'
- The load of hemoglobin kills the tubular
epithelium, leading to renal shutdown and death.
- The HbS of sickle cell disease
confers substantial resistance to malaria.
- Sickled cells adhere to endothelium in
areas of low O2 tension.
- Potassium loss from these hypoxic RBCs
kills the parasites.
- Although there are a number of effective
medications to treat malaria,
- Mosquito control remains the mainstay of
public health intervention.
- Two strains of the bug, P. vivax and P.
ovale, have developed an interesting strategy for surviving
periods when no mosquitoes are in the environment. They go into a latent
phase (hypnozoites) and can persist in the hepatocytes for months and some
people think even years. This feature probably accounts for relapses of
malaria long after the initial infection.
|
|
Wow, I never knew malaria was such a fascinating
disease. What's next?
Back
|